


Misplaced coronavirus complacency
With many Australians and New Zealanders living their lives as they did pre-pandemic, but with severe international travel restrictions, it is easy to understand the current complacency about COVID-19. This complacency is misplaced.
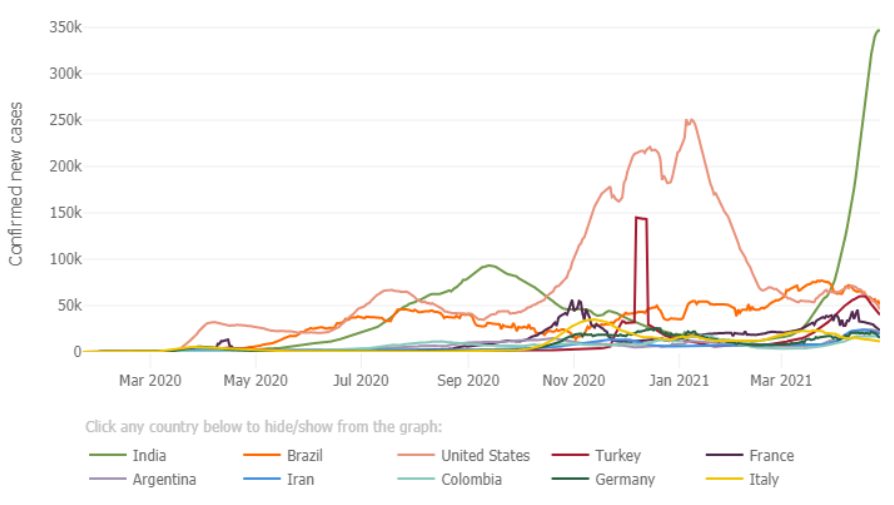
Reported worldwide daily infection rates are now higher than they have ever been and could top 1 million within a week or so. This is due to COVID-19 overwhelming some countries’ health systems. They are probably more under-reported now than they have ever been. Reported daily death rates are again climbing rapidly though still just under their peak in January, but again the true death toll is much higher than reported and, in any event, even the reported death rate in the new wave will soon surpass the January peak. The following graphic shows the seven day moving averages of confirmed new cases in the most affected countries as at 29 April 2021, courtesy of John Hopkins University COVID website.
Some countries that had major infections and are quickly rolling out their vaccination programs have reduced and/or stabilised their infection rates, while other countries are seeing rapid rises in infections. Currently the hardest hit is India, and what is happening there is instrumental for actuaries to understand why our profession must not become complacent. This pandemic has a long way to go and the current ‘new normal’ in Australia and New Zealand is the best we are likely to get for some years. Other countries with more open international borders must either adopt the Australian and New Zealand measures to control the pandemic or face ongoing health and economic disruption for an extended time.
What is happening in India? For a start, India’s reported numbers have always been a fraction of the true numbers. This is true in many countries. This is not intended as a criticism of India. India also has the largest pharmaceutical manufacturing industry in the world and was exporting vaccines to the rest of the world until mid-April, so what is happening in India is immediately going to affect vaccination programs everywhere. Whether cessation of vaccine exports from India are due to the pandemic, the beefing up of its own vaccine program, or overseas supply chain issues1 is unclear. But even if India beefed up its vaccination program 5-fold from 3 million a day to 15 million a day, it may not make much difference if, as it now appears many current vaccines will not confer much immunity to some newer strains of the virus.
India’s coronavirus testing rate is low compared to many other countries. Most recently it recorded around a high 20% positive test rate, (US is 4%, Turkey 16% and France 9%)2.
Currently the northern states of India are being hit harder than the southern states. The northern states had a relatively cold late winter and spring so that could be one underlying cause of the new wave. Another is religious holidays and a third being mass unrestricted and unmasked political gatherings. But this is India. Similar occasions last year did not cause such an outbreak. The real problem is the so-called ‘double mutant’, B.1.617 variant and probably several other mutations that either have not been given names or have not yet been recognised3. Maharashtra state, capital Mumbai, the financial capital of India, along with Delhi are currently being hit hard by this new wave. Mumbai is being particularly affected and this is concerning because reports in mid-June 2020 indicated that then some 57% of the population of Mumbai’s slum regions had been infected by the first wave of the virus4.
By then, Mumbai residents, at least in its slums, had either reached or would have soon reached herd immunity. Fortunately, back then, the slum dwellers’ rates of serious infection and/or death were quite low. Currently, the sequencing that has been performed (and its less than 5% of tests) suggest that the double variant mutation is predominate in this new wave. It seems obvious, although the Indian Department of Health have not yet verified this, that people who should have had immunity due to an earlier infection are being re-infected. Although this will provide a nightmare for epidemiologists and governments around the world, this reality is going to have to be faced. Like the flu, common colds and other cold-like coronavirus infections, this virus mutates often. Some new mutations will not be recognised by the memory T cells of the immune systems of people who have previously had an earlier form of that virus or have been vaccinated against an earlier form.
Considering that more than one thousand trillion viral particles are being produced every day, it is understandable that each day there will be new mutations of this single stranded DNA particle. Most of these mutations will not be more infectious than the parent strain and so are of little consequence. Every now and then a mutation will be significantly more infectious and therefore will eventually become dominant. Often, in the past, viruses burnt themselves out if the dominant (most infectious) mutation also killed nearly all those it infected or, paradoxically, was relatively harmless and so conferred herd immunity. But these days with the advanced state of medical intervention capabilities, the medical circumvention of the mortality consequences of a lethal, predominantly infectious mutant strain of a virus will only eventually cause the implosion of medical facilities – unless population controls reduce the R0 of the virus to below one. This was the initial objective in Australia and New Zealand.
The Wall Street Journal reported that the double mutant strain actually has 13 mutations but gets its name from two mutations similar to those seen separately in other variants. In other variants, one mutation is associated with making the virus more infectious and appears better at evading antibodies, while the other is similar to one variant that has shown signs of being able to sidestep some of the body’s immune responses.
Scientific opinion is somewhat more muted. The following is a verbatim quote from AlJazeera (19 April 2021):
|
“In some districts in Maharashtra state – home to Mumbai and epicentre of the current wave that’s triggered fresh lockdown-like rules – the prevalence of this variant was more than 60%, according to Anurag Agrawal, director of the state-run Council of Scientific and Industrial Research’s genomics institute that’s conducting sequencing. The B.1.617 was present in samples from about 10 Indian states and while the percentage may vary, it was expected to rise as “it has two critical mutations that make it more likely to transmit and escape prior immunity,” Agrawal said. Both mutations are known to decrease – although not completely eliminate – the binding of the antibodies created by infection and vaccination, according to Jesse Bloom, an associate professor for genome sciences and microbiology at the University of Washington. “Mutations at sites E484 and L452 have been observed separately, but this is the first major viral lineage that combines the two,” said Bloom. “I do think that this new viral variant is important to monitor.” “We did the math – we do believe that a lot of the increase in the reproduction number can be explained by these mutations,” Nithya Balasubramanian, the head of health-care research at Bernstein India, told Bloomberg TV this week. “ |
Last week in India, the double mutant variant made up 70% of all infections that were sequenced. In Australia, the double mutant variant made up 40% of the samples collected over the week ended 15 April, compared with 16.7% a month earlier. It accounted for 66.7% of samples from New Zealand for the week ended 8 April, up from 20% a month ago.
Hospitals in the epicentre of this latest outbreak in India are completely overloaded with patients dying before they can get treatment. One doctor working at one of these hospitals explained why. He said that this mutation of the virus attacks the lungs almost immediately a patient gets infected. It means that within two days of infection, the patient could require oxygen to survive5. This is well before the body can mobilise its immune responses to counteract the infection. This is probably why the virus is causing critical illness in younger people, who normally could have been expected to survive an earlier COVID-19 infection because their immune system would have had enough time to react and counteract the infection before the lungs were affected. It is too early to determine whether this mutation of the virus is more deadly than before, because of the low rate of sequencing. But it probably is, given people are building funeral pyres in the car park of the Delhi crematorium, and other crematoriums are experiencing similar behaviour. According to scientists advising the Wall Street Journal, the double mutant version has significantly higher mortality rates in younger people than the original version of the virus. Early Indian statistics suggest people aged 26-44 with the double mutant strain are making up 40% of the admissions to hospital and contributing to 10% of the deaths6. Comprehensive statistics will eventually become available. But actuaries don’t always have time to wait for comprehensive statistics. We sometimes must form our judgements on very limited data!
Since these Indian strains of the virus are sometimes infecting the lungs before the nasopharyngeal region virus clumps or particles must have been breathed into the lungs directly. This suggests that some mutations of the virus are either forming tiny clumps in droplets or are aerosolising as individual virus particles. It was initially assumed that SAR-COV-2 would form much larger clumps in droplets which would generally get caught in the nasopharyngeal region. This aerosolisation of the virus would explain why the reverse-transcription polymerase chain reaction (RT-PCR) serology tests on patients presenting at hospitals sometimes gives a negative result. Incidentally, Chinese hospital doctors in the very early stages of this pandemic in Wuhan also complained of the RT-PCR test giving false negatives and they had to change to CT Scan diagnoses to determine the presence of the virus in the lungs. Indian hospital doctors are also adopting this regime.
This article is intended to make actuaries in Australia and New Zealand less complacent about the COVID-19 pandemic. I hope that those in our great profession in other countries will also read this. The SARS-COV-2 virus was never going to go away any time soon. It will evolve into an annual threat and maybe international travel will not be the same as it was pre-pandemic for at least a decade. Businesses will have to continually evolve to new modes of operation, and many will never regain their pre-pandemic modes of operation.
References1 – There are significant supply chain issues currently in vaccine manufacturing. Vaccines are made from several components and equipment that are manufactured in many countries. The US Defence Production Act is being used by the US to divert parts of the vaccine supply chain that are made in the US for its own vaccine manufacturing purposes. Also, although the WTO has requested a temporary suspension of pharmaceutical vaccine patents the US, UK and Europe are refusing to do so. This means that poorer countries can’t make their own generic copies of major vaccines. Adar Poonawalla – head of India’s Serum Institute “If we are truly united in beating this virus on behalf of the vaccine industry outside of the US I humbly request you to lift the embargo of new material exports out of the US so that vaccine production can ramp up.” https://www.washingtonpost.com/world/2021/04/24/coronavirus-vaccine-us-anger-inequality/ 2 – Data derived from https://www.worldometers.info/coronavirus/#repro In Nagpur it reached 30 per cent, and in Chandrapur it got as high as 50 per cent https://www.abc.net.au/news/2021-04-13/how-double-mutant-coronavirus-complicated-indias-outbreak/100059714 3 – For example the B.1.618 a West Bengal variant has 4 mutations to the spike protein that appear to increase its infectivity. https://www.downtoearth.org.in/news/health/-double-mutant-covid-19-variant-colonises-lungs-directly-evades-rt-pcr-experts-76609 4 – https://www.bbc.com/news/world-asia-india-53576653 5 – Anirban Dolui, a public health expert associated with West Bengal government – “The conventional SARS-CoV-2 strain usually colonises the nasopharyngeal region where the body’s immune system counters it and stops it from directly accessing the lungs. However, the double mutant variant was believed to evade the nasopharyngeal region and colonise the lungs directly”. https://www.downtoearth.org.in/news/health/-double-mutant-covid-19-variant-colonises-lungs-directly-evades-rt-pcr-experts-76609 6 – https://timesofindia.indiatimes.com/city/ranchi/double-mutant-variant-uk-strain-lethal-for-youngsters/articleshow/82134576.cms |
CPD: Actuaries Institute Members can claim two CPD points for every hour of reading articles on Actuaries Digital.




