


COVID-19 4 March – Status Update
The state of the coronavirus continues to develop across the globe. Author and speaker at the upcoming Summit, Alex Stitt, provides a status update of his Covid-19 article from February.
This article provides a brief update on the status of that epidemic. The article is the opinion of the author only and is endorsed by no one else. It’s informed by a range of sources which the author believes to be authoritative, using worldometers.info/coronavirus/ as a major reference point.
FAST MOVING WORLD
In this fast-moving epidemic world, the ‘hard facts’ in this article are obsolete even before I submit it for review prior to publication. Please read them as point-in-time observations and look through the detail to the trend they’re trying to report.
ESTABLISHED FACTS
The virus has been formally named (take a deep breath) ‘Severe acute respiratory syndrome coronavirus 2’ or SARS-CoV-2 for short.
The disease it causes has been formally named ‘Coronavirus disease’. Who’d have thought? Or COVID-19 for short.
On 28 February, WHO raised their risk assessment to “Very high at a global level”. They have stopped short of declaring a pandemic. The kind say that’s because there is still some hope of containing the outbreak – and there is some validity to this view. The unkind say it’s purely political.
On 27 February the Australian Government declared they were treating the outbreak as a pandemic and activated their Emergency Response Plan.
DISEASE DYNAMICS
Human to human spread of the infection is well established. Authorities are starting to have difficulty tracing the origin of some infections. Because …
The latency (or incubation) period and period of non-symptomatic infectivity of COVID-19 is not yet well established, but there are more than sufficient instances of non-symptomatic infection across the globe to infer there is a non-trivial latency period.
I‘ve seen zero data or commentary attempting to quantify post-recovery infectivity. Other viral diseases are known to have non-trivial post-recovery infectivity. Live virus can shed from body fluids and faeces after the immune system has controlled the virus (i.e. after the individual has recovered).
The latency challenge is: … what practical steps can be taken to guard against infection (by infected persons and their touched objects) when those persons are unaware they’re infectious?
Given the latency, the ‘lockdown’ challenge is: … will it work, or is it too late?
- The China and Diamond Princess cases point to aggressive lockdown being effective at containment. The big question is whether aggressive lockdown is possible except in China and on the Diamond Princess.
- Conversely the China, North Italy and Iran outbreaks point to the difficulty in locking down before the disease has escaped to the next locality.
The quarantine challenge is: … how long is enough?
- No one has a solid answer to this yet.
- Quoted “central” infectivity periods are 5 to 14 days, but the range may be a few days to much longer.
- There appear to be outlier instances of nearly 4 week infectivity.
- It should be no surprise there is a range that varies by individual carrier. Some HIV carriers remain infectious and asymptomatic throughout their lives.
- But, to date, the 14 day quarantine appears to be broadly effective.
In the UK, it has been stated that the outbreak will likely take 2-3 months to peak after the first local human-to-human spread, and will then take another 2-3 months to taper off.
GLOBAL SPREAD / PANDEMIC PROGNOSIS
The following table, at 2 March for data at 1 March, is intended to be illustrative of six things:
- It’s a rapidly moving situation.
- No matter what the politics, the outbreaks appear to meet the definition of a pandemic.
- There are multiple “waves” of the outbreak happening across different locations at different stages of development.
- It’s possible that, in some locations, the outbreak is being contained.
- It’s not clear in other locations that containment will succeed.
- It’s highly unlikely the outbreaks won’t spread further in both range (localities affected) and scope (proportion of those in a locality affected).
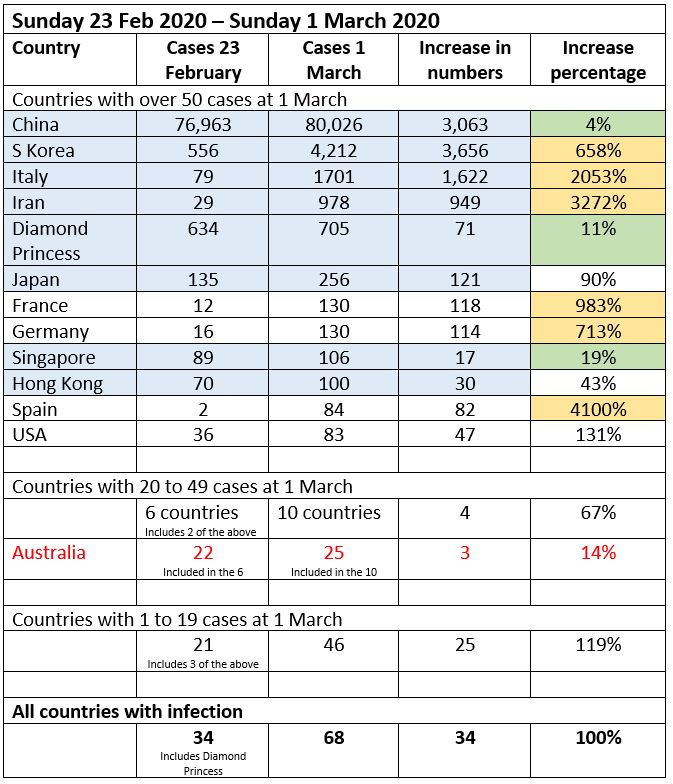
- Blue lines indicate where (my assessment) sustained human-to-human spread is occurring or has occurred.
- Green change cells indicate places where containment may have been achieved (for the time being).
- Yellow change cells indicate locations where (my assessment) a local outbreak is underway in its very early stages (comparable to China between 23 January and 30 January).
- As a flash update, as of 3 March, p.m. data: Cases are up 7% (78% ex-China), deaths are up 6%, recoveries are up 15% (100% ex-China), countries with any infection are up 18% and countries with over 50 cases are up 25%.
DISEASE OUTCOMES – MORTALITY
COVID-19 is a fatal disease. Overall, case fatality rates (CFRs) are estimated at 2% to 3%, although some raw figures appear to point to much higher CFRs. Conversely, it is reported that outside Hubei Province, the China outbreak has CFRs of circa 1%. Some (non-Chinese) medical sources attribute this lower rate to early and aggressive treatment of the sick.
COVID-19 is particularly savage for older age groups. The data in this table is a large study from China.
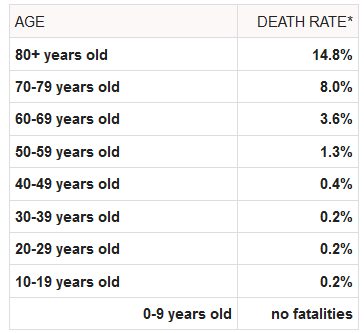
The extraordinarily low fatality rate and low levels of symptoms in the very young is a mystery the medical profession is rushing to try and understand.
Much is made of the co-morbidity fatality rates.
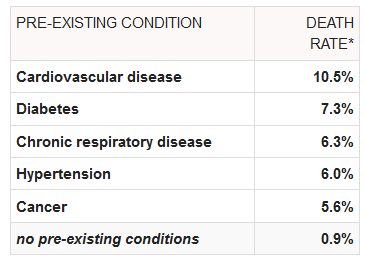
Given the low under 60’s CFRs and the very high over 70s CFRs, I’m not putting much stock in these early numbers. Age-and-co-morbidity specific rates would be needed to make any solid prognostication. That said, particular care should be taken with older persons and persons with the noted pre-existing conditions.
It may be possible that males are more susceptible than females and their CFR’s higher. Again, without more detailed By-age-and-sex specific rates, this may merely reflect classical human mortality and morbidity differences by sex.
DISEASE OUTCOMES – MORBIDITY
COVID-19 presents a wide range of severities in the sick, but a significant proportion of the sick are very sick, needing hospitalization, with a non-trivial proportion needing intensive care.
From the 3 March (p.m.) data, with a total of 92,880 cases, the breakdown of severity is:
- 37% (34,056) have mild infection.
- 7.7% (7,162) have a serious infection.
- 52% (48,494) have recovered.
- 3.4% (3,168) have died.
From this it can be seen that 83% of active infections are mild and 17% serious.
However, in some localities the outcomes are worse than this overall picture. For instance, in Italy, 46% of active cases are hospitalized and 25% of those (10% of all active cases) are in intensive care.
ECONOMIC PROGNOSIS
To a large extent, the economic prognosis depends on what you believe is the prognosis for the spread and depth of the COVID-19 outbreak.
To help guide us, the Brookings Institute have released a paper by McKibbin & Fernando modelling seven scenarios for the country-by country economic impact. The paper can be downloaded at: brookings.edu/20200302_COVID19.pdf.
Scenarios 1 to 3 assume no spread of COVID-19 beyond China. Scenarios 4 to 6 assume one-off pandemics of varying severity. Scenario 7 assumes a mild, annually occurring pandemic of COVID-19, much like seasonal influenza.
For Australia, the headline model outcomes for scenarios 4 to 7 are:
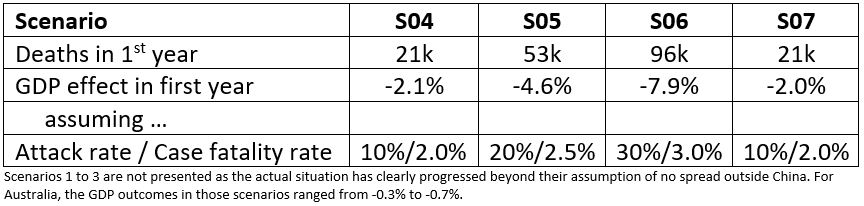
It’s worth noting (my understanding) that the three scenarios quoted assume a full-fledged pandemic with the characteristics briefly noted (eg S06, that 30% of populations become infected). This, in turn, implies that public health / containment measures have limited efficacy. The development of outbreaks to-date generally point to good outcomes from public health / containment measures. The scenario results should be interpreted accordingly.
For comparison, the seasonal ‘flu infects about 250,000 Australians each year and kills up to 1000.
INVESTMENT MARKET PROGNOSIS
To a large extent, the investment market prognosis depends on what you believe the market believes is the prognosis for the spread and depth of the COVID-19 outbreak.
To date, the investment market response has been very muted, dropping about 8% from record highs and then recovering somewhat.
The only way this commentator can rationalize the outcome to date is that the market believes the outbreaks will be contained, there will be no pandemic and no material economic impact.
CPD: Actuaries Institute Members can claim two CPD points for every hour of reading articles on Actuaries Digital.




