The near future of healthcare – FOHS 3 Plenary report
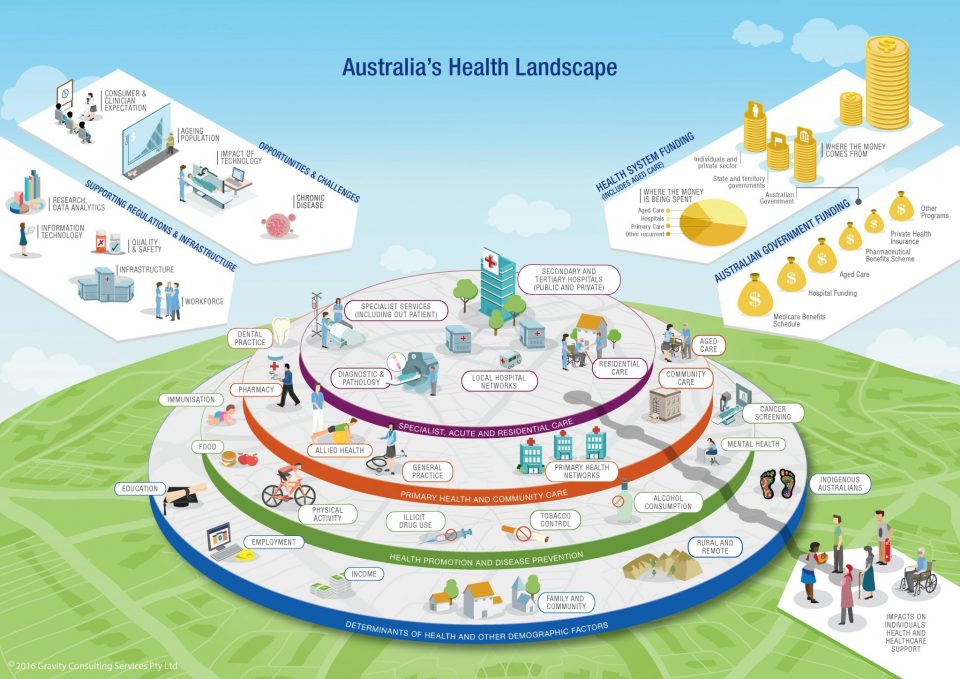
Plenary 3 covered a range of discussions around ‘the near future of healthcare’. A shift towards a patient-centric healthcare system measured by ‘value-add’ rather than cost was a major theme.
When Plenary 3 started after lunch, there was a full house in attendance. Everyone in the room was refreshed and engaged when Jamie Reid from Finity opened the session by introducing the three speakers: Leanne Wells the CEO of Consumer Health Forum of Australia (CHF), Sue Williams from Cabrini Health Australia and Dr Jananie William, Senior Lecturer in Actuarial Studies, Australian National University. With a focus on the near future of healthcare, the topics of public versus private and patient centred healthcare were the focus alongside many of the other themes of the day, as explored in this FOHS Overview article.
Leanne Wells spoke about the need and urgency of transitioning towards a patient and person centred healthcare system.
“Practices needs to be respectful of and responsive to the preferences, needs and values of patients” at the point of care and advocating for policy. Being a health advocate for many years, she outlined what high value care is to consumers:
access – the right care, at the right time in the right place
safety and high quality – people assume that only safe care will be offered but there’s a lot of variation
[ability to] navigate the system – “between a quarter to a third of consumers have difficulty navigating the system”
affordability
choice and control
An improved system needs to reframe the thinking around care. What we need to do shift to is an approach of rather than ask “what’s the matter with you?”, practitioners should ask “what matters to you? what will make a difference to you?”
To reduce the complexity, we should “re-gear the system to provide more preventative and accessible healthcare services in a community setting”.
People need to be better supported with more “sign posts” and navigation to support the best pathways of care. It’s not until people start using the system that they realise how complex it is and we need to improve this.
The issue and challenge in the current system was explored from a provider’s perspective by Sue William of Cabrina, a not-for-profit health service provider offering a comprehensive range of health services. Sue highlighted many of the problems in our system out-of-pocket payment, multiple bills for a single admission, shortage in healthcare service workforce, and challenges of rolling out electronic health records. Perhaps most notably, she highlighted the increasing competition from the public system – which offers patients no out of pocket costs.
To address this public competition, the private hospital operators, along with private health insurers need to react. Sue outlines a few key necessary responses:
Conversations between PHIs and hospital groups need to be more than just about price
The DRG model is outdated
A better approach could be to capitate services to providers, with risk adjustment
This can offer both shared risk and incentives for the providers to shift care out of a hospital setting
Tackling out of pocket issues is incredibly important – particularly for a value for money perspective, but is complex
There are many outsourced service providers, even within hospitals (e.g. radiology and pathology)
Potential ACCC issues when discussing prices with contracted medical staff
New models of care can respond to both patient preferences and improve quality while reducing costs. But to get providers to channel care out of hospital requires medical engagement, trust and strong relationships between medical practitioners and out of hospital care providers.
Further, vertical integration can offer greater control of supply chain to lower costs and create a seamless and easy-to-navigate experience for the patient. However, all these transitions would take a lot of work for everyone involved to agree and for the system to be implemented.
Maternal care trends
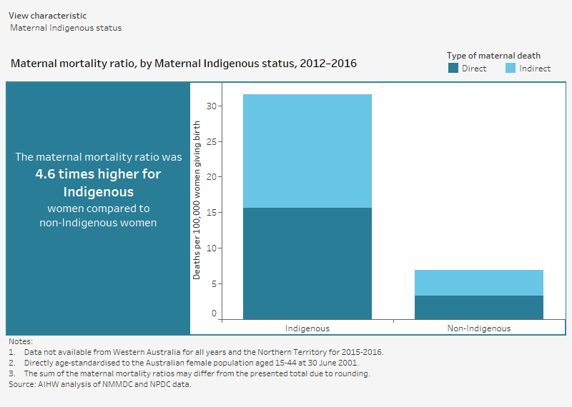
Narrowing down to the maternal health, Dr. Jananie William from ANU also highlighted the increasing competition from the public system to the private as well as the disparity in healthcare.
The equity issue is quite pronounced in maternal care. Indigenous women have a 4.6 higher rate of maternal death compared to non-indigenous women.
While maternal care is often cited as the reason that many women purchase PHI, there is a trend towards greater usage of the public system. This is broadly in line with overall uptake of PHI (which has been decreasing in younger groups).
“90% of woman stayed within the same (public or private) system from one birth to the next”
Jananie’s research showed the differences between women with private health insurance to those without and the outcome has more to do with their social economical background, rather than anti-selection.
Read more
See a summary of other Plenary sessions written by Brendan Pon, Lulu Wang, Nora Lam and Zachary Tirrell